De Souza et al in the BMJ (http://www.bmj.com/content/351/bmj.h3978) wrote a piece which is another stone in the backyard of government guidelines and conventional nutritionists who are still advising patients to eat a low fat diet to reduce their risk of CVD. In this comment we will challenge the link between saturated fats and CVD but not the issues of saturated fat replacement or trans fat.
Saturated fat consumption, scientific interest and political issues
Fat consumption in populations is subjected to a continuous scrutiny from researchers and government agencies since the aftermath of World War 2. This is mainly the consequence of the lipid heart hypothesis formulated by Ancel Keys and never confirmed since.This scrutiny suffered all the bias of retrospective or prospective non-interventional epidemiological studies about diet and CVD:
-Very poor quality of diet analysis and questionnaires
-No control group and a lot of confounding parameters
-Weak correlations and very low absolute risk differences
-Wide range of metabolic responses among individuals to intake of carbs / lipids / proteins
-Ignorance of the type of fat and especially the amount of industrially produced trans fats
-Selection of countries and/ or avoidance of those with high intake of saturated fats and low CVD rates like France or Spain.
To illustrate the precedent bias let me review the selection process of the studies as shown in Figure N°1 of the paper (http://www.bmj.com/content/351/bmj.h3978). From 20413 studies in the database only 41 were selected because of lack of information, low quality, and other insufficiencies. For instance from the 445 studies resulting of a process of eligibility based on the full text, 372 were excluded because
-They did not assess saturated fat exposure
-They did not measure outcomes of interest
-They duplicate data from previous publications
-They did not present a measure of associations
-They have an inappropriate study design.
There is more, the GRADE (http://www.gradeworkinggroup.org/index.htm) evidence profile of quality is very low for all the comparisons done in the selected studies (http://www.bmj.com/content/bmj/suppl/2015/08/11/bmj.h3978.DC1/sour025275.ww5_default.pdf).
What are the findings?
Another time I have to insist on a critical point in human observational studies about diet: mortality is crucial. As there is no experimental design but only a retrospective or prospective follow up of a cohort crude mortality is the more evident and unfalsifiable event that can be reported. Without any effect on mortality observational studies should be taken with extreme precautions for further conclusions. Figure number 2 which is displayed below illustrates very precisely how saturated fat are neutral on different risks ans d the great heterogeneity of studies on CHD and saturated fats..
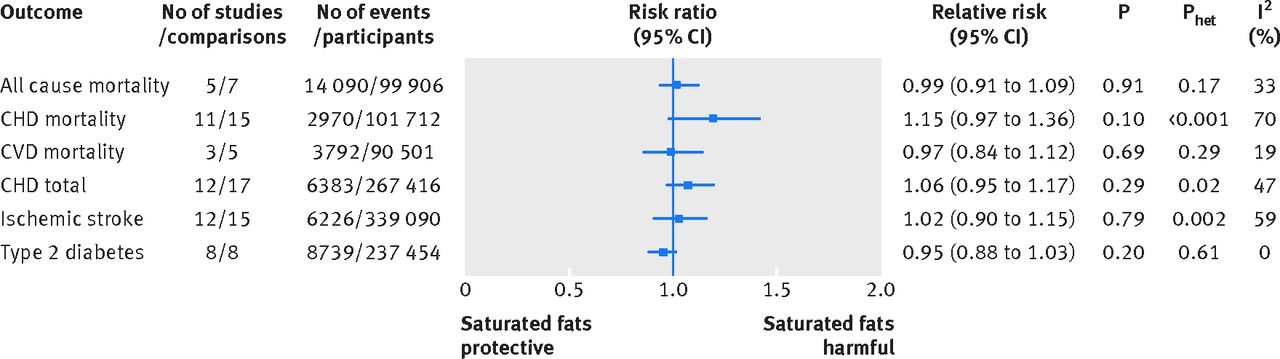
What is obvious on this figure is that observational studies about saturated fats are not to be replicated. In order to assess eventually the discrete evidence of saturated fats only interventional studies of real foods in humans should be undertaken. Those future studies should also integrate a new model of diet assessment based on wireless technology and collection of data.
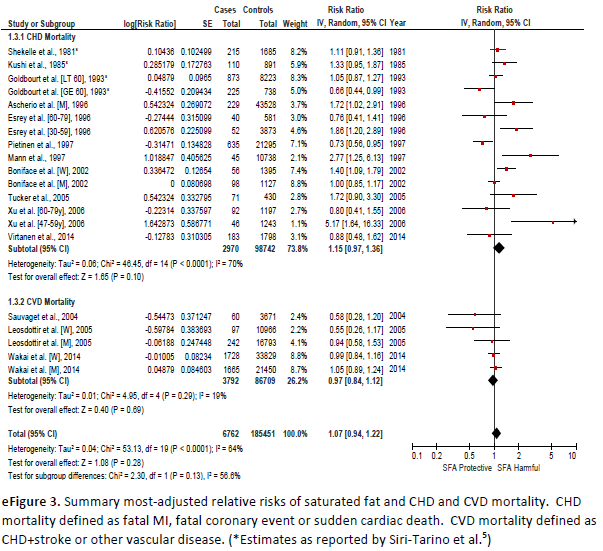 In this supplementary Figure one can look at an usual specific trend in observational studies on saturated fats and CVD. One can observe a small trend in increased CHD mortality and a small beneficial trend on stroke mortality which lead to a summed neutral effect. How is it possible in such a class of disease where atheroma plays a great causal role? No clear answer could be formulated to this fact and another time only interventional high quality controlled studies should allow more detailed observations.
In this supplementary Figure one can look at an usual specific trend in observational studies on saturated fats and CVD. One can observe a small trend in increased CHD mortality and a small beneficial trend on stroke mortality which lead to a summed neutral effect. How is it possible in such a class of disease where atheroma plays a great causal role? No clear answer could be formulated to this fact and another time only interventional high quality controlled studies should allow more detailed observations.
Recently the number of papers by nutrition specialists who doubt or challenge results of studies about saturated fats and CVD has increased because the statistical reality as assessed by meta-analysis or recalculating old data is indeed against any detrimental effect of saturated fats on cardiovascular health.
Eventually authors concluded that in this synthesis of observational evidence they found nuclear association between the hiring take of saturated fats and all-cause mortality, CHD , CHD mortality, ischemic stroke, or type 2 diabetes among apparently healthy adults.
Limitations of this paper are very well discussed and they shed a mixed light on nutritional studies especially in the past era.
Atheroma and CVD are complex issues which are not caused by fat (nor cholesterol) in your plate
For sure we are at the beginning of the end of a myth. The only surprise is the slowness of the process id est the extraordinary conservatism of the scientific community about the diet heart hypothesis. No doubt that economic interests (the low fat industry, the sugar industry and at large the agrofood industry) and the traditional reluctance to change of highly centralised bureaucracy are key explanations for exceptional lasting of this myth, but enough is enough, because those advices are not neutral but deleterious to populations which follow them and consequently do not engage in actual and efficient prevention of CVD.



Aucun commentaire:
Enregistrer un commentaire